Locations:

Insights on a still-maturing subspecialty from one of its largest U.S. programs
At the national level, vascular medicine is on the cusp of adolescence as a subspecialty, with board certification exams having been offered by the American Board of Vascular Medicine since just 2005.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Yet Cleveland Clinic’s vascular medicine program was established in the mid-1950s, making it one of the nation’s first such programs and allowing it to grow into one of the largest.
Cleveland Clinic’s experience in the subspecialty provides a window into the discipline as it transitions to maturity. That was the thinking behind a presentation by Cleveland Clinic vascular medicine specialist Maya Serhal, MD, at last fall’s American Heart Association meeting. Highlights of the presentation — titled “Characterizing the Practice of Vascular Medicine at an Academic Medical Center” — are captured below.
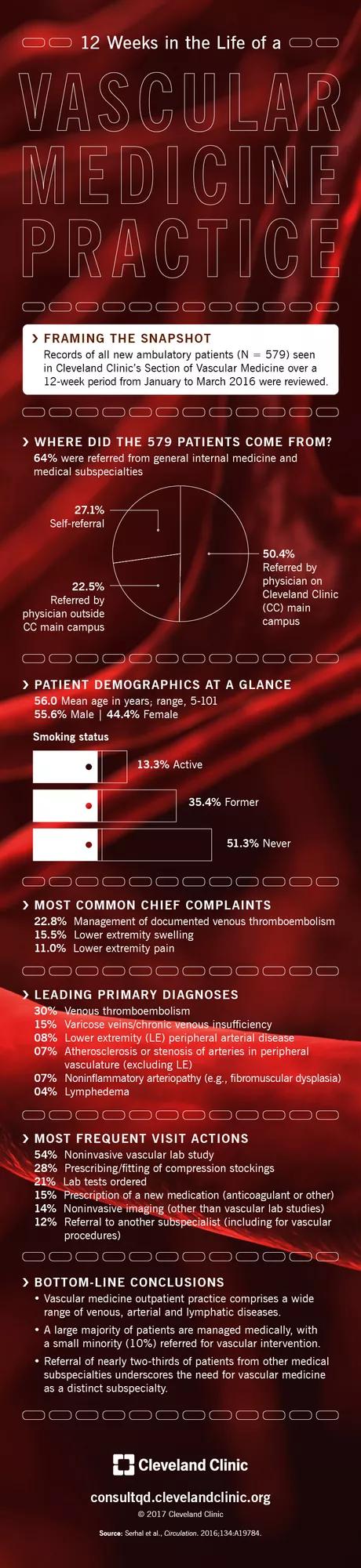
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/a77e7a3c-ba8e-4f03-bfe3-9c9a4d00eaf8/16-HRT-2471-Vasc-Med-infographic-FNL_jpg)
The abstract of the presentation is below:
There is increasing recognition of vascular medicine as a distinct subspecialty of internal medicine and cardiology. There are currently few vascular medicine training programs nationwide. We sought to characterize the nature of an outpatient vascular medicine practice at an academic center. We present a single center registry and medical record review of new outpatient evaluations seen in vascular medicine clinic in 13 weeks (1/25/2016-4/22/2016) seen by 11 vascular medicine staff physicians. Reason for consultation, diagnosis and visit actions were captured. Five hundred and seventy nine new patient evaluations were reviewed. Mean patient age was 56.0 ± 16.2 years (range 5-101 years), 44.4% were male. General internal medicine, cardiology and other subspecialty medicine represented the majority of referrals (45.7%); vascular surgery represented 2.4%. Most common chief complaints were management of venous thromboembolism (VTE), lower extremity (LE) swelling and LE pain. Most common visit primary diagnoses were: VTE, varicose veins/chronic venous insufficiency, LE peripheral artery disease or critical limb ischemia, atherosclerosis or stenosis of non-LE arteries, non-inflammatory arteriopathies and lymphedema. Most common visit actions include non-invasive vascular lab study (54.2%), prescribing or fitting compression stockings (27.9%), laboratory testing (21.1%), prescribing new medication (anticoagulant or other) (15.4%), other non-invasive imaging (14.3%) and referring to another subspecialist (12.3%). Only 10.2% of patients were referred or scheduled for vascular intervention. Vascular medicine practice encompasses a broad spectrum of diseases of the venous, arterial and lymphatic systems. A minority of new patients were referred for vascular intervention, highlighting the importance of medical management in the treatment of vascular disease. A majority of patients seen by vascular medicine specialists at an academic center were referred from internal medicine or its subspecialty providers. These data support vascular medicine as a distinct subspecialty, independent of internal medicine and cardiology.
Advertisement
Advertisement

A sampling of outcome and volume data from our Heart & Vascular Institute

Concomitant AF ablation and LAA occlusion strongly endorsed during elective heart surgery

Large retrospective study supports its addition to BAV repair toolbox at expert centers

Young age, solid tumor, high uptake on PET and KRAS mutation signal risk, suggest need for lobectomy

Surprise findings argue for caution about testosterone use in men at risk for fracture

Residual AR related to severe preoperative AR increases risk of progression, need for reoperation

Findings support emphasis on markers of frailty related to, but not dependent on, age

Provides option for patients previously deemed anatomically unsuitable